
 Testosterone Cypionate, often referred to as “Test C” or “Test Cyp”, is one of a handful of the injectable, esterified Testosterone variants. Test C has an expanded half-life due to the cypionate ester which is attached to the testosterone molecule. There are little differences between Test E and Test C in terms of half-life, medical application, and convenience; Test E and Test C are used identically.
Testosterone Cypionate, often referred to as “Test C” or “Test Cyp”, is one of a handful of the injectable, esterified Testosterone variants. Test C has an expanded half-life due to the cypionate ester which is attached to the testosterone molecule. There are little differences between Test E and Test C in terms of half-life, medical application, and convenience; Test E and Test C are used identically.
The biggest difference between the two testosterone variants are their country of origin. Test E was originally released in the prescription market in Europe, and Test C was created in America in response. During the golden age of body building, it seems that bodybuilders tended to use Test C more-so than Test E simply to support an American made product. Like Test E, the same rules apply:
Medical applications of Testosterone Cypionate typically include treatment of hypogonadism or andropause, which is preceded by hypogonadism. This disorder happens over time with age in all men and is often referred to as “male menopause”, but can also happen prematurely as a developmental disorder, disease, or injury. The average weekly dose for men undergoing testosterone replacement therapy (TRT) tends to be between 75mg – 100mg a week of Testosterone Cypionate. The most commonly recommended dose for a first time cycler seeking to utilize Testosterone Cypionate for muscle size and strength is typically 500mg a week for roughly 8-20 weeks. A more intermediate cycle might see doses upwards of 750mg-1000mg a week.
The general consensus regarding side-effects is that they are dose dependent. That is, the higher the dose, the higher the likelihood of both androgenic and estrogenic side effects. In the presence of 5α-reductase, testosterone will convert to DHT, and likewise, when the aromatase enzyme is present, testosterone will convert to oestradiol which can bind to the estrogen receptors and perpetuate estrogenic side-effects. See below.
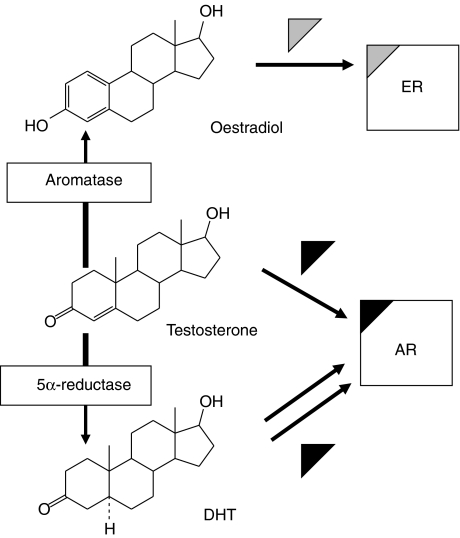
The conversion of testosterone to DHT commonly leads to an enlarged prostate, or the most feared DHT side-effect, male-pattern-balding (MPB). MPB should only be a concern to those who tend to have a genetic predisposition to this trait. That is, if you are going to go bald, DHT will expedite that process. In order to combat the conversion off testosterone to DHT, users may opt to include a “5-alpha reductase inhibitor” such as Finasteride or Duasteride. These compounds inhibit the reductase enzyme from converting testosterone to DHT.
Due to the conversion from testosterone to estrogen, the user may experience estrogenic side effects such as water retention, breast tenderness or breast tissue development (gynecomastia), high blood pressure, high LDL cholesterol, low HDL cholesterol. There are two avenues a user might take to counteract the conversion of testosterone to estrogen.
The athlete may use of a compound such as Aromasin, a “Type-I Aromatase Inhibitor”, often referred to as a “suicide inhibitor”. This drug works by attaching to the aromatase enzyme and permanently deactivating it. Other benefits of this drug include increased IGF-1 production, and even an increase in testosterone, however only in men not endogenously injecting it. Another option is the use or a “Type-II Aromatase Inhibitor” such as Arimidex. Arimidex competes with testosterone for the aromatase enzyme, and effectively lowers the conversion of testosterone to estrogen. However, upon cessation of Arimidex administration, the aromatase enzyme is then free to begin converting testosterone to estrogen again leading to what many call the “estrogen rebound”. Arimidex is also harsher on cholesterol levels than Aromasin.
As a side note, often, users may hear that taking Tamoxifen (Nolvadex) will suffice in counteracting estrogenic side effects. This is true, but only to a certain extent. Nolvadex will only bind to the estrogen receptor, blocking estrogen from doing so and effectively blocking estrogen related side-effects, but the problem of excess estrogen still exists. It is for this reason that Nolvadex should only be used in emergencies to block gyno from progressing, but the user should remedy the actual cause of gyno, high conversion of testosterone to estrogen, with Aromasin or Arimidex.
In summary, much like Testosterone Enanthate, Testosterone Cypionate is one of the most proven and one of the most well researched compounds utilized in AAS cycles. As such, it’s efficacy and versatility make it one of the most popular injectables on the mainstream and black-market. However safe, all users body’s are different and should proceed with caution when considering any AAS cycle. Frequent blood work and doctor supervision is always recommended.